Advances in Neurosurgery
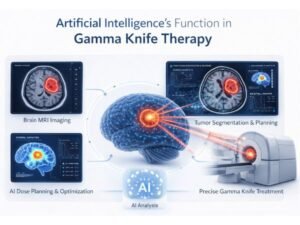
How Artificial Intelligence Is Transforming GAMMA KNIFE Treatment for Vestibular Schwannoma
Topics Table of Contents How Artificial Intelligence Is Transforming GAMMA KNIFE Treatment for Vestibular Schwannoma Artificial Intelligence’s Function in GAMMA KNIFE Therapy Every phase of