

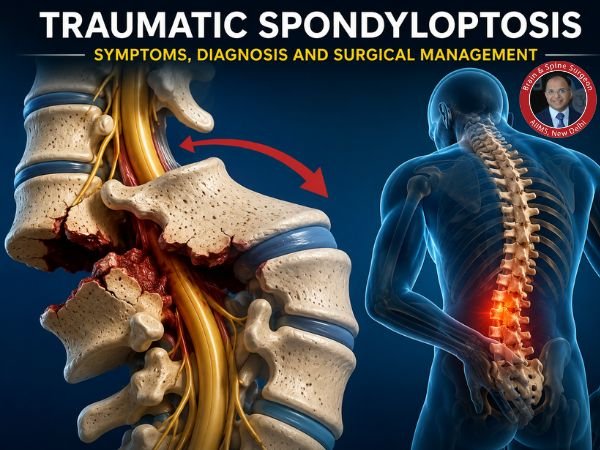
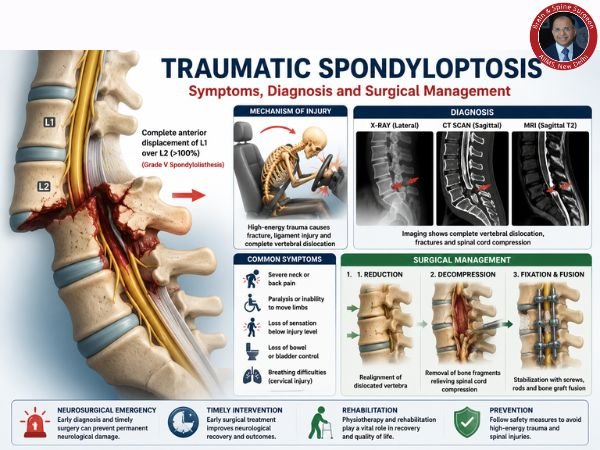
One vertebra is completely dislocated over another in traumatic spondyloptosis, an uncommon but serious spinal injury. This disorder, which is frequently referred to as a “grade V spondylolisthesis,” is caused by high-impact trauma, such as crush injuries, falls from heights, or car crashes. If not treated quickly, this neurosurgical emergency could result in severe neurological impairments, including paralysis.
Everything you need to know about traumatic spondyloptosis will be covered in this guide, from symptoms and diagnosis to sophisticated surgical management.
Traumatic Spondyloptosis: What Is It?
Complete displacement of one vertebra over another, either forward, backward, or sideways, is referred to as traumatic spondyloptosis. This displacement frequently results in compression or transection of the spinal cord and produces extreme instability of the spine.
It most frequently happens in:
- Neck (cervical spine)
- Mid-back, or thoracic spine
- Lower back, or lumbar spine
Traumatic Spondyloptosis Causes
High-energy trauma is usually the cause of this condition, including:
- The most frequent cause of traffic accidents
- Falls from a considerable height
- Construction or industrial mishaps
- Sports-related injuries (uncommon but conceivable)
The force used results in full spinal dislocation, fractures, and destruction of ligaments.
Traumatic Spondyloptosis Symptoms
The degree of damage and degree of spinal cord involvement determine the symptoms.
Typical Symptoms Include:
- Severe neck or back discomfort
- Paralysis, or the inability to move limbs
- Sensation loss below the site of damage
- Loss of control over the bowels and bladder
- Improper posture or spinal malformation
- Breathing problems (particularly with cervical injuries)
Signs of an Emergency
Get medical attention right away if you observe:
- Abrupt paralysis
- Loss of consciousness following trauma
- After an accident, severe spinal discomfort
Traumatic Spondyloptosis Diagnosis
To stop additional harm, an early and precise diagnosis is essential.
Clinical Assessment
- Neurological testing to evaluate sensory and motor abilities
- Evaluation of spinal stability
Imaging Examinations
X-rays
- Preliminary evaluation of vertebral alignment
CT Scan
- A thorough assessment of bone dislocations and fractures
MRI Scan
- Crucial for evaluating soft tissues, ligaments, and spinal cord damage
MRI is especially crucial for assessing the degree of spinal cord damage or compression, which informs therapy choices.
Categorisation and Severity
The most serious type of spinal injury is traumatic spondyloptosis, which frequently includes:
- Total dislocation of the vertebrae (>100%)
- Spinal instability in multiple columns
- High chance of irreversible brain damage
Handling Traumatic Spondyloptosis
First Emergency Response
- Spinal immobilisation
- Stabilisation of breathing, circulation, and airways
- Using spinal boards or cervical collars
Treatment of Traumatic Spondyloptosis with Surgery
The main and most effective treatment for this illness is surgery.
Objectives of Surgery
- Spine realignment (reduction)
- Release the spinal cord’s compression
- Use implants to stabilise the spine
- Preventing more brain damage
Typical Surgical Methods
1. Decompression of the Spine
Removal of disc material or pieces of bone that are pushing against the spinal cord.
2. Diminished Dislocation
To restore normal anatomy, dislocated vertebrae must be carefully realigned.
3. Fusion and Fixation of the Spine
- Using plates, rods, and screws to stabilise the spine
- Bone grafting to encourage vertebral fusion
4. Combined Methods
Both anterior (front) and posterior (back) surgical techniques may be necessary in complex instances.
Healing and Rehabilitation
Recuperation is dependent upon:
- Spinal cord injury severity
- Treatment time
- The patient’s general health
Included in Rehabilitation Are:
- Physical therapy
- Occupational therapy
- Pain control
- Psychological assistance
Improving results and quality of life is largely dependent on early rehabilitation.
Prognosis
- Following surgery, patients without spinal cord injuries may make a full recovery.
- Severe brain damage may leave a person permanently disabled.
- Results are greatly improved by early surgical intervention.
Preventive Advice
Although not every situation can be avoided, you can lower risk by:
- Observing traffic safety regulations
- Putting on helmets and seat belts
- Stay away from dangerous activities when playing sports
- Ensuring adherence to workplace safety regulations
In Conclusion
A serious spinal injury that necessitates prompt medical attention and skilled neurosurgical care is traumatic spondyloptosis. Many patients can have better results and a higher quality of life because of developments in surgery and therapy.
Seeking prompt examination by a qualified neurosurgeon is crucial if you or a loved one has suffered a serious spinal injury.
FAQ’s
1. Is it possible to die from traumatic spondyloptosis?
Indeed, it is a serious illness that may be fatal, particularly if there is spinal cord damage or breathing compromise.
2. Can someone who has spondyloptosis walk again?
The degree of spinal cord injury determines this. While some individuals regain their ability to move, others might become permanently paralysed.
3. Is surgery necessary all the time?
Indeed, surgery is typically required to stabilise the spine and stop additional brain injury.
4. How much time does it take to recover?
Depending on the extent of the damage and rehabilitation efforts, recovery may take several months to years.
5. What is the surgical success rate?
Timing, severity, and patient health are some of the variables that affect surgical success. Results are greatly improved by early intervention.
Sources
- https://pubmed.ncbi.nlm.nih.gov/42028504/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC13101750/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC11465537/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC11465537/
- https://pubmed.ncbi.nlm.nih.gov/18764746/
- https://pubmed.ncbi.nlm.nih.gov/25768668/
- https://pubmed.ncbi.nlm.nih.gov/39385287/