Overview
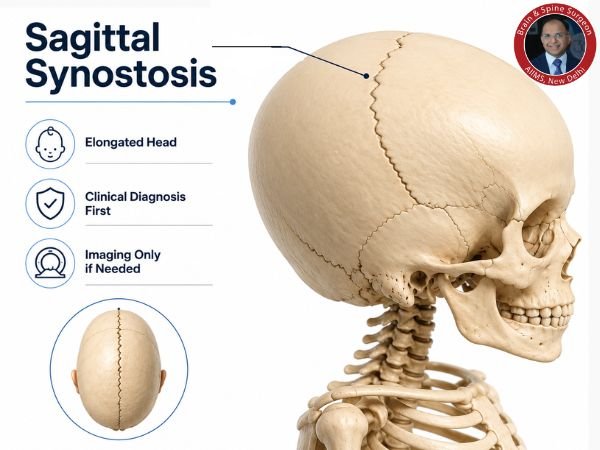
The most prevalent type of craniosynostosis, in which one or more of the fibrous joints (sutures) connecting a baby’s skull bones fuse prematurely, is isolated sagittal synostosis. Scaphocephaly, an extended head shape, can result from this early fusion, which interferes with normal skull growth.
Parents and other carers frequently wonder if X-rays are required to diagnose sagittal synostosis. This blog examines the diagnostic process, the use of imaging, and the situations in which sophisticated scans or X-rays may or may not be necessary.
Isolated Sagittal Synostosis: What Is It?
The sagittal suture follows the midline from the front to the rear of the skull. When this suture fuses too soon:
- Sideways expansion of the skull is not possible.
- That makes up for it by getting longer from front to back.
- As a result, the head form becomes narrow and elongated.
Characteristics:
- Boat-shaped head with a long, thin skull
- Prominent forehead (frontal bossing)
- Temples that are narrow
- The sagittal suture may have a ridge.
How is the Diagnosis of Sagittal Synostosis Made?
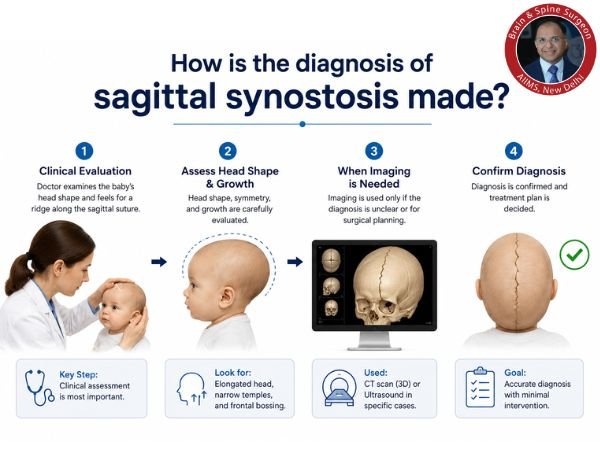
1. Clinical Assessment (Most Crucial)
The majority of the time, a skilled neurosurgeon’s physical examination serves as the primary basis for the diagnosis.
An expert will evaluate:
- Shape and symmetry of the head
- Ridging that is palpable over the sagittal suture
- Growth trends of head circumference
- Developmental benchmarks
Key Point: In classic cases, sagittal synostosis can be diagnosed without imaging by a skilled physician.
2. Are X-rays Required?
Brief Response: Generally, no.
Fused sutures were traditionally identified via X-rays of the skull. However, a number of restrictions have caused their function to drastically diminish:
X-ray Limitations:
- Low sensitivity in the first few months of life
- Inadequate suture visualisation in comparison to contemporary imaging
- Radiation exposure (although minimal)
Current Practice: X-rays are rarely necessary and are typically avoided, particularly when the clinical diagnosis is evident.
3. When Is Imaging Necessary?
Imaging may be advised in specific circumstances, even though it is not necessary in many cases:
a) Unusual Head Shape
If the diagnosis is unclear or the shape of the skull is not typical.
b) Planning Prior to Surgery
Detailed imaging aids in the following prior to corrective surgery:
- Verifying the joining of sutures
- Knowing the anatomy of the skull
c) Differential Diagnosis
To differentiate from circumstances such as:
- Flat head syndrome, or positional plagiocephaly
- Different forms of craniosynostosis
Top Imaging Techniques
1. 3D Reconstruction from a CT Scan
- The gold standard for verification
- Gives a thorough suture visualisation
- Aids in the planning of surgery
CT scans are used sparingly, though, because they entail radiation.
2. Ultrasound (for Babies)
- Radiation-free and non-invasive
- Beneficial for younger babies with open fontanelles
- Operator-dependent but becoming more and more popular
3. MRI (Seldom Used)
- Usually not required for suture assessment
- May be applied if there is a suspicion of related brain disorders
Experts Preferences for Clinical vs. Imaging-Based Diagnosis
The focus of contemporary neurosurgical practice is:
- Prioritise clinical diagnosis
- Prevent needless radiation
- Utilise imaging only when it alters treatment
This strategy guarantees:
- The child’s safety
- Cost Effective
- Quicker decision-making
Why Avoid Unnecessary X-rays?
- Children are more radiation-sensitive.
- Long-term dangers are increased by repeated imaging.
- X-rays frequently don’t provide useful diagnostic information.
Conclusion: X-rays can be safely avoided if the diagnosis is clear clinically.
When Should Parents Seek Expert Advice?
Get a medical assessment if you observe:
- An unusually formed head
- Increasing the head’s length relative to its width
- The top of the skull has a ridge
- Developmental delay (uncommon but significant)
Better treatment results are possible with early diagnosis, particularly if surgery is necessary.
Overview of Treatment
The severity and age at diagnosis determine the course of treatment:
- Mild instances: Observation
- Surgical correction in moderate to severe cases
- Surgery with little invasiveness (in younger infants)
- Remodelling of the open cerebral vault
The best outcomes come from early intervention, usually before the age of one year.
In Conclusion
The way isolated sagittal synostosis is diagnosed has changed dramatically. Nowadays, unnecessary invasive imaging, particularly X-rays, is mostly avoided, and clinical competence is crucial.
CT scans and other advanced imaging are only used in specific situations where they have a direct impact on treatment choices. Safety, precision, and the best possible results are guaranteed by this patient-centered approach.
See a licensed neurosurgeon as soon as possible if you think your child’s head shape is abnormal for an accurate assessment and direction.
FAQs
1. Is it possible to identify sagittal synostosis without X-rays?
Indeed. Most of the time, a skilled physician can make the diagnosis with just a physical examination.
2. Is a CT scan necessary every time?
No, CT scans are used seldom, mostly for surgical planning or confirmation.
3. Can infants be harmed by X-rays?
Even if the radiation dose is minimal, avoiding needless exposure is advised, particularly for young children.
4. Which imaging method is the safest?
Because it doesn’t use radiation, ultrasound is the safest method, and it’s especially helpful for small babies.
5. When should a diagnosis be made?
For best therapy results, this should ideally happen during the first few months of life.
6. Is brain development impacted by this condition?
Brain development is normal in the majority of isolated cases. Severe untreated cases, however, could be dangerous.
7. Is surgery always necessary?
Not all the time. While many cases require surgery for both functional and cosmetic repair, mild cases may merely require monitoring.
Sources
- https://pubmed.ncbi.nlm.nih.gov/16187144/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC10887665/
- https://pubmed.ncbi.nlm.nih.gov/22801186/
- https://journals.lww.com/jcraniofacialsurgery/abstract/2012/07000/magnetic_resonance_imaging_in_isolated_sagittal.127.aspx
- https://pubmed.ncbi.nlm.nih.gov/38396475/
- https://pubmed.ncbi.nlm.nih.gov/22872242/
- https://www.semanticscholar.org/paper/Diagnosis-of-isolated-sagittal-synostosis%3A-are-Agrawal-Steinbok/e8e551e228774413a2a77bf1d39a5fc017bfb400