
An uncommon and aggressive form of non-Hodgkin lymphoma that only affects the brain, spinal cord, eyes, or leptomeninges is called primary central nervous system lymphoma (PCNSL). Although radiologists and neurosurgeons are familiar with the conventional imaging findings of Primary CNS Lymphoma, its unique radiological presentations can be very difficult to diagnose because they frequently resemble other brain tumours or illnesses.
For early diagnosis, prompt treatment, and better patient outcomes, it is essential to comprehend these unusual imaging patterns.
Primary CNS Lymphoma: What is it?
A malignant tumour called primary CNS lymphoma develops from lymphocytes in the central nervous system. It does not initially affect other body parts, in contrast to systemic lymphoma.
Important Features:
Immunocompromised people are most frequently affected, however immunocompetent persons might also experience it.
Usually involves deep brain areas like:
- The basal ganglia
- Callosum corpus
- Periventricular areas
Typical PCNSL Radiological Features
PCNSL typically displays the following on imaging tests like MRIs and CT scans:
- Uniform augmentation of contrast
- CT scan hyperdense lesions
- MRI with restricted diffusion
- Minimal necrosis, particularly in those who are immunocompetent
Making a first diagnosis is frequently aided by these common characteristics.
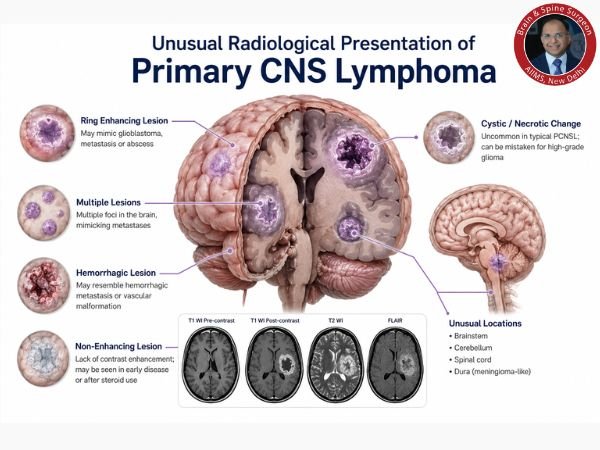
Unusual Primary CNS Lymphoma Radiological Presentations
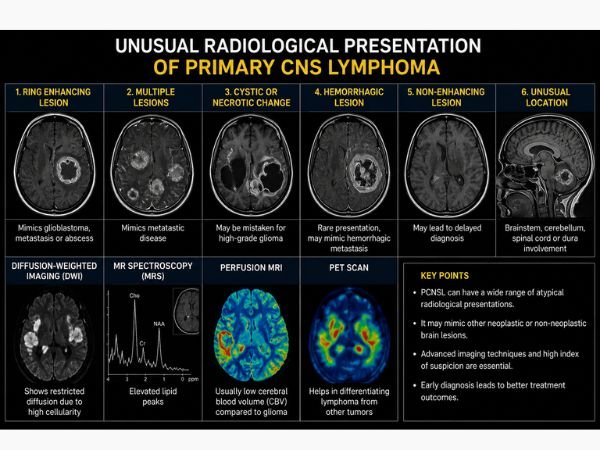
Atypical imaging results from PCNSL can occasionally cause misunderstanding with other neurological disorders.
1. Lesions that Enhance Rings
- Can resemble glioblastoma, metastases, or brain abscess.
- More prevalent in patients with weak immune systems
2. Lesions with Many Foci
- Numerous lesions dispersed across the brain
- Might mimic tumours that have spread.
3. Cystic or Necrotic Alterations
- Uncommon in traditional PCNSL
- May result in a false diagnosis of high-grade glioma.
4. Hemorrhagic Wounds
- It is rare for the tumour to bleed.
- May mimic hemorrhagic metastases or vascular abnormalities.
5. Lesions That Don’t Enhance
- A delayed diagnosis may result from a lack of contrast enhancement.
- Observed in the early stages of the illness or following steroid use
6. Involvement of Odd Places
- Brainstem
- Cerebellum
- The spinal cord
- Dura (meningioma-like)
What Causes These Abnormal Presentations?
Atypical imaging appearances are caused by a number of factors:
- Corticosteroid use prior to imaging
- Immunocompromised condition, such as HIV/AIDS
- Aggression and tumour biology
- Disease stage at presentation
Diagnostic Difficulties
Unusual radiological signals may result in:
- Inaccurate or delayed diagnosis
- Unnecessary surgical procedures
- Inadequate treatment of the illness
Among the differential diagnoses are:
- Multiform glioblastoma
- Metastases to the brain
- Tuberculosis
- An abscess in the brain
- Multiple sclerosis is one example of a demyelinating condition.
Advanced Imaging Techniques’ Function
Advanced imaging modalities are frequently employed to increase diagnosis accuracy:
1. DWI, or Diffusion-Weighted Imaging
Demonstrates limited diffusion as a result of high cellularity.
2. MR Spectroscopy
Elevated lipid peaks are symptomatic.
3. MRI with Perfusion
In contrast to high-grade gliomas, it usually has low cerebral blood volume (CBV).
4. A PET Scan
Aids in distinguishing lymphoma from other tumours.
Early and Accurate Diagnosis is Crucial
It’s crucial to diagnose PCNSL early because:
- It responds quite well to radiation and chemotherapy.
- Typically, surgery is not the main course of treatment.
- Prognosis can deteriorate if treatment is delayed.
Overview of Treatment
Usually, treatment consists of:
- High-dose chemotherapy with methotrexate
- Radiation therapy for the entire brain (in certain instances)
- Immunotherapy and targeted therapy (new choices)
Prognosis
The following factors affect PCNSL prognosis:
- Age of the patient
- Immune status
- Early diagnosis
- Reaction to treatment
Many individuals experience remission with prompt therapy.
In Conclusion
One of the most important diagnostic challenges in neurosurgery and neuro-oncology is the uncommon radiological appearance of primary CNS lymphoma. By being aware of these unusual imaging patterns, one can assure prompt treatment, avoid unnecessary operations, and avoid misdiagnosis.
Early contact with a neurospecialist is crucial for correct diagnosis and successful treatment of patients with unexplained neurological complaints.
FAQ’s
1. Why is it challenging to diagnose primary CNS lymphoma?
Confusion and a delayed diagnosis can result from unusual radiological findings that resemble other brain disorders.
2. Can a brain tumour be confused with PCNSL?
Indeed, it may mimic glioblastoma or metastasis, particularly if it appears as ring-enhancing or necrotic lesions.
3. Is a biopsy required to make a diagnosis?
Indeed, especially in unusual situations, a brain biopsy is frequently needed to confirm the diagnosis.
4. Does the usage of steroids impact diagnosis?
Indeed, corticosteroids can change imaging results and temporarily decrease the tumour, making diagnosis more challenging.
5. Is it possible to treat primary CNS lymphoma?
Indeed, chemotherapy and radiation therapy are very effective in treating it, especially if it is discovered early.
6. Who is more susceptible to PCNSL?
People with impaired immune systems, such as those with HIV/AIDS or recipients of organ transplants, are more vulnerable.
7. Can PCNSL be confirmed by MRI alone?
No, MRI offers powerful hints, but histological confirmation is necessary for a conclusive diagnosis.
Sources
- https://pubmed.ncbi.nlm.nih.gov/33527818/
- https://pubmed.ncbi.nlm.nih.gov/16193386/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC9163949/
- https://www.ncbi.nlm.nih.gov/books/NBK545145/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC4757149/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC9072256/
- https://radiopaedia.org/articles/lymphomas-of-the-central-nervous-system