Rare but potentially dangerous brain vascular anomalies are called intracranial dural arteriovenous fistulas (dAVFs). They have to do with abnormal artery-vein connections in the dura mater, the brain’s outermost layer. In contrast to congenital arteriovenous malformations (AVMs), dAVFs are usually acquired lesions that may arise later in life as a result of venous thrombosis, trauma, infection, or surgery. Certain dAVFs might result in life-threatening bleeding or severe neurological impairments if treatment is not received.
A Dural Arteriovenous Fistula: What Is It?
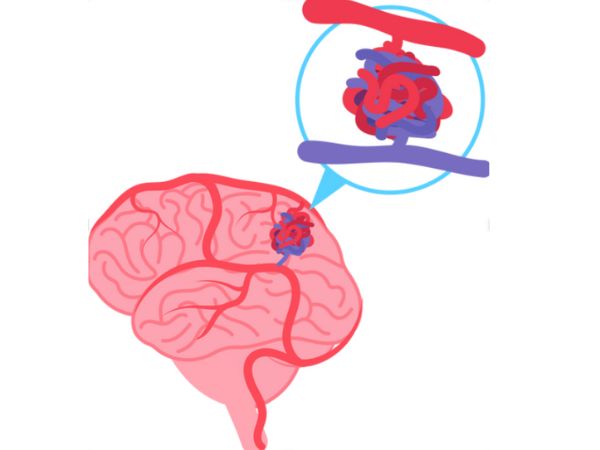
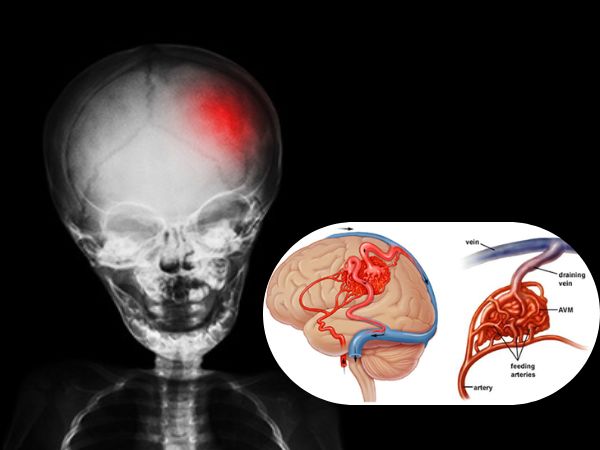
An irregular direct connection between the meningeal arteries and the dural venous sinuses or cortical veins is known as a dural arteriovenous fistula (dAVF). Blood normally travels from arteries to capillaries and finally to veins. This capillary bed is bypassed in a dAVF, allowing high-pressure arterial blood to enter the low-pressure venous system directly. Depending on the drainage pattern and location, this can cause neurological symptoms, venous congestion, or haemorrhage.
Reasons/Causes and Dangers
A number of factors are linked to the development of dAVFs, though their exact cause is not always evident:
- Thrombosis of the dural sinuses
- Head injuries
- Neurosurgical techniques
- Infections
- States of hypercoagulability
With no obvious gender preference, they are most frequently observed in middle-aged to older persons.
The symptoms of the Intracranial Dural Arterivenous Fistula are as follows:
The size, location, and blood flow pattern of dAVFs all affect the symptoms. While some may show up with serious neurological problems, others may stay asymptomatic and be found by chance.
Typical signs and symptoms include:

- A headache
- Hearing a rhythmic sound in the ear is known as pulsatile tinnitus.
- Visual disruptions
- Seizures
- Deficits in the cranial nerve
- Dementia-like symptoms or cognitive decline
- Haemorrhage inside the brain (in high-grade fistulas)
Classification
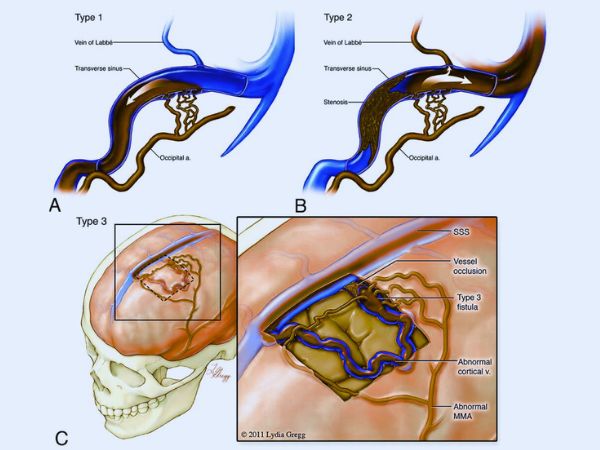
Based on their venous drainage patterns and haemorrhage risk, dAVFs are categorised using the Cognard and Borden categorisation systems.
Classification by Borden:
- Type I: Low risk drainage into a venous sinus
- Type II: Retrograde cortical venous drainage into a venous sinus (moderate risk)
- Type III: High-risk direct cortical venous drainage
Classification by Cognard:
Varies according to venous drainage patterns and flow direction, ranging from Type I (benign) to Type V (most aggressive).
Diagnosis
In order to avoid complications, early diagnosis is essential. The imaging modalities that are employed include:
- For preliminary evaluation, magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA) are helpful.
- Computed Tomography Angiography (CTA): May reveal abnormal veins and swollen feeding arteries.
- The gold standard for diagnosis is digital subtraction angiography (DSA), which offers fine-grained visualisation of the venous drainage, feeding arteries, and fistula.
Options for Treatment
The dAVF’s categorisation, location, and symptoms all influence the therapy option. The goal of treatment is to restore normal venous drainage and close the abnormal link.
Embolisation of Endovascular
- A minimally invasive procedure in which the fistula is sealed shut by administering embolic chemicals via a catheter.
- Frequently the initial course of treatment.
Resection by Microsurgery
- Used when embolisation is impractical or fails.
- Involves cutting the fistula directly during surgery.
Gamma Knife Surgery, or stereotactic radiosurgery
- An approach for non-invasive therapy that works especially well for residual or low-flow fistulas.
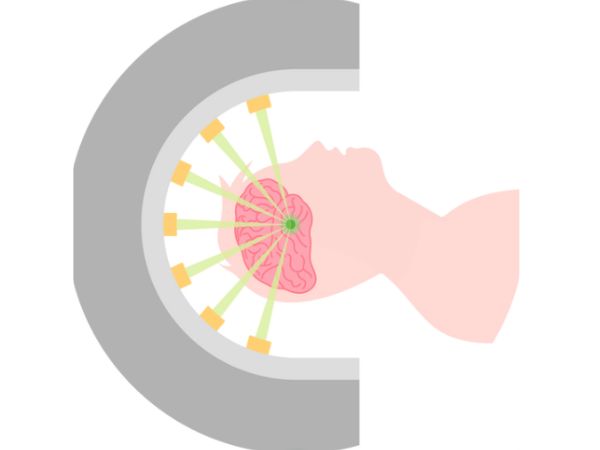
Intracranial Dural Arteriovenous Fistulas with Gamma Knife Surgery
A type of stereotactic radiosurgery known as “gamma knife” (GKS) uses concentrated, high-dose radiation beams to precisely target the abnormal vascular connections inside the dura while preserving the surrounding healthy brain tissue.
How It Operates:
- Through damage to endothelial cells and vessel wall thickening, the radiation causes the unusual vessels to gradually close over the course of months to years.
- It is usually applied to individuals who are not a good candidate for invasive procedures or to low-grade or persistent dAVFs following unsuccessful embolisation.
Gamma Knife Surgery Indications for dAVFs:
- Tiny, persistent fistulas following embolisation
- Deeply seated or inaccessible surgical sites
- Low-risk dAVFs that are asymptomatic or only slightly symptomatic
- Comorbidities in patients that raise the risk of surgery
Benefits:
- Non-invasive
- Procedure for outpatients
- Short recovery period
- Suitable for use in conjunction with additional therapies
Limitations:
- Effect delayed: Total obliteration may take six to thirty-six months.
- Not appropriate for high-grade or quickly developing fistulas with cortical venous reflux.
- The evaluation of obliteration requires routine follow-up imaging.
Prognosis and Follow-Up
The fistula’s classification and drainage pattern determine the prognosis. While low-risk dAVFs can be seen, high-risk ones need to be treated right away.
Follow-up consists of:
- DSA or serial MRI/MRA
- Preventing recurrence
- Neurological evaluation
In most situations, a favourable outcome can be achieved with appropriate diagnosis and treatment. For certain cases, Gamma Knife Surgery has demonstrated exceptional obliteration rates with little adverse consequences.
In conclusion
Vascular abnormalities known as intracranial dural arteriovenous fistulas are complicated but curable. For the best results, a multidisciplinary strategy including radiation oncologists, neurosurgeons, and interventional neuroradiologists is essential. For some forms of dAVFs, Gamma Knife Surgery has become a potent non-invasive treatment option, particularly when embolisation or traditional surgery may be unsafe or insufficient.
Early contact with a specialised neurosurgery team can significantly impact treatment outcomes and quality of life if you or a loved one is diagnosed with a dAVF.
Sources:
- https://pmc.ncbi.nlm.nih.gov/articles/PMC8013238/#sec10
- https://pmc.ncbi.nlm.nih.gov/articles/PMC5435465/
- https://radiopaedia.org/articles/dural-arteriovenous-fistula
- https://www.ahajournals.org/doi/10.1161/strokeaha.115.008228
- https://my.clevelandclinic.org/health/diseases/dural-arteriovenous-fistula-davf
- https://www.mayoclinic.org/diseases-conditions/dural-arteriovenous-fistulas/symptoms-causes/syc-20364280
- https://link.springer.com/article/10.1007/s13760-022-02133-6