Craniopharyngioma: What is it?
An important medical problem that may necessitate lifelong care is a craniopharyngioma. Over time, almost half of all surgically excised tumours recur. Numerous illnesses brought on by craniopharyngiomas persist even after the tumour has been removed.
What distinguishes a pituitary adenoma from a craniopharyngioma?
Hormone function can be impacted by pituitary adenomas and craniopharyngiomas. Craniopharyngiomas are found close to the pituitary gland, while pituitary adenomas are tumours that originate from the pituitary gland itself. Despite the fact that both tumours are benign, pituitary adenomas are often less aggressive than craniopharyngiomas.
Histology and Types
Two primary histological subtypes exist:
- Children are more likely to have Adamantinomatous Craniopharyngioma (ACP). characterised by calcifications, cystic components, and frequently a more infiltrative character.
- PCP, or papillary craniopharyngioma, is usually observed in adults. less calcified and more firm, frequently leading to superior surgical results.
Pathogenesis and Causes
Although the precise source is unknown, it is believed that craniopharyngiomas develop from the remains of Rathke’s pouch, an embryonic structure that gives birth to the anterior pituitary.
- Mutations in the CTNNB1 gene (β-catenin pathway) are frequently linked to the amantinomatous type.
- BRAF V600E mutations have therapeutic implications and are associated with papillary type.
Signs and symptoms
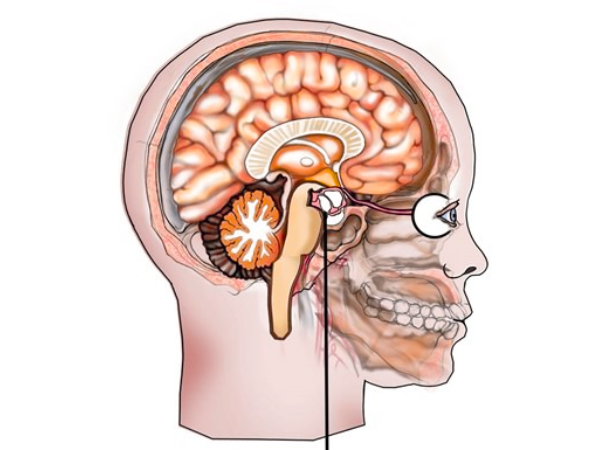
Because craniopharyngiomas are located close to important brain areas, they can cause a range of symptoms:
- Visual abnormalities (caused by the optic chiasm being compressed)
- A headache
- Imbalances in hormones (causd by pituitary malfunction)
- Children’s growth delays
- Fatigue, memory problems, and obesity (because of hypothalamus involvement)
- If the tumour blocks the cerebrospinal fluid channels, hydrocephalus may result.
Diagnosis
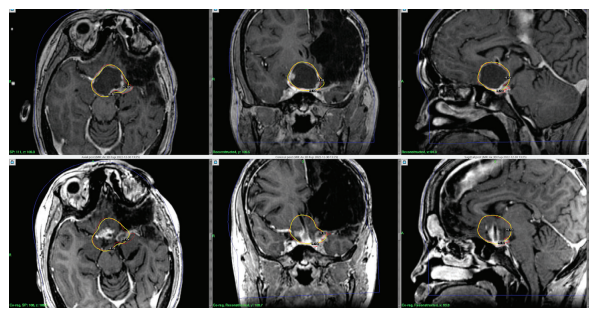
- Imaging:
- The gold standard is MRI, which shows calcifications, cystic/solid mass, and the connection to surrounding structures.
- A CT scan can make calcifications easier to see.
- Endocrine Assessment:
- Pituitary hormone testing, both baseline and dynamic, is crucial.
Options for Treatment
A comprehensive approach is necessary for the management of craniopharyngiomas. Maximum tumour control while maintaining neurological and endocrine function is the aim.
Surgery
The standard of care is still surgical removal. Methods consist of:
- Craniotomy, or transcranial surgery
- For midline lesions, the endoscopic endonasal approach (EEA) is becoming more and more popular.
Adherence to key structures may make complete excision difficult.
Radiation therapy
Radiotherapy after surgery is frequently used when:
- The tumour has been partially removed.
- Recurrence happens.
- Surgery is very risky.
Proton treatment, stereotactic radiosurgery, and conventional fractionated radiation are available.
Radiosurgery with Gamma Knife for Craniopharyngiomas
Gamma Knife Radiosurgery: What is it?
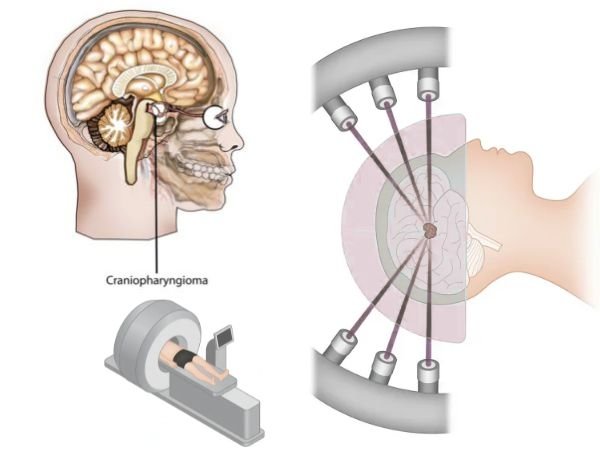
Gamma Knife radiosurgery is a non-invasive stereotactic procedure that spares the surrounding brain tissue while precisely giving high doses of radiation to the tumour. Small to medium-sized lesions close to important structures respond especially well to treatment.
Indications or Signs and symptoms of craniopharyngiomas
- After subtotal resection, residual tumour
- Recurrence following the initial procedure
- Patients who are medically inoperable
- Near optical equipment, tumours (with appropriate dose planning)
- Before GKRS, cystic components may be shrunken or aspirated.
Craniopharyngioma Primary Gamma Knife Radiosurgery
Gamma Knife radiosurgery can be used as the main treatment in some circumstances without surgical resection, especially in:
- Tumours that are little (<3 cm)
- Clearly clear margins
- Tumours that don’t produce immediate symptoms like hydrocephalus or profound blindness
- Patients in poor overall health or at high risk for surgery
Benefits:
- Minimally intrusive or invasive
- Maintains brain function
- Outpatient treatment or brief hospitalisation
- Shorter recuperation period
- Repeatable if necessary
Restrictions:
- Large, symptomatic, or cystic tumours with mass effect are not the best candidates.
- Risk of visual deterioration or delayed hypopituitarism (rare with proper dose)
Results and Outlook
It is possible to achieve long-term tumour control with the right care. But even after treatment, endocrine dysfunction frequently continues. Hormonal testing and MRI imaging are necessary for lifelong monitoring.
Rates of Survival:
- Overall 5-year survival: greater than 90%
- In carefully chosen patients, the Gamma Knife tumour control rate is 80–90%.
In conclusion
Despite being benign, craniopharyngiomas present a number of difficulties because of their location and effect on essential activities. The greatest results are guaranteed by a customised strategy that combines stereotactic radiosurgery, such as Gamma Knife, radiation, and surgery. Primary Gamma Knife radiosurgery is a safe and efficient substitute for surgery in carefully selected patients, particularly where neurological and endocrine function preservation is the goal.
Sources:
- https://www.ncbi.nlm.nih.gov/books/NBK459371/#:~:text=Craniopharyngioma%20is%20a%20rare%2C%20virtually,visual%20disturbances%2C%20and%20endocrine%20disturbances.
- https://www.mayoclinic.org/diseases-conditions/craniopharyngioma/symptoms-causes/syc-20581521
- https://my.clevelandclinic.org/health/diseases/22989-craniopharyngioma
- https://en.wikipedia.org/wiki/Craniopharyngioma
- https://www.hopkinsmedicine.org/health/conditions-and-diseases/craniopharyngioma
- https://www.aans.org/patients/conditions-treatments/craniopharyngiomas/
- https://academic.oup.com/edrv/article-abstract/27/4/371/2355225?redirectedFrom=fulltext
- https://www.sciencedirect.com/science/article/pii/S0003426624001082