Overview
One of the most typical kinds of brain tumors is a meningioma, which develops from the meninges, which are the protective coverings that surround the brain and spinal cord. Some meningiomas can be more aggressive, although the majority are benign and grow slowly. Atypical meningioma, which is categorised as WHO Grade II, is one such variation. Compared to normal (benign) meningiomas, these tumours have a higher chance of recurrence and need to be managed more carefully.
Atypical Meningioma: What Is It?
A brain tumour that develops from the meninges but exhibits characteristics that make it more aggressive than a conventional (Grade I) meningioma is known as an atypical meningioma. These cancers:
- Possess a greater cell division rate.
- Can infiltrate adjacent brain tissue
- They are more likely to return following therapy.
- Represent roughly 15–20% of all meningiomas.
Reasons and Risks
Although the precise cause of atypical meningiomas is unknown, the following risk factors are linked to their development:
- Exposure to radiation
- Hereditary disorders such as neurofibromatosis type 2 (NF2)
- Effects of hormones, particularly in women
- Meningioma family history
Signs and Symptoms
Symptoms of atypical meningiomas depend on their size and location in the brain or spinal cord. Typical signs and symptoms include:
A headache
- Seizures
- Issues with vision
- Deafness
- Numbness or motor weakness
- Changes in personality or cognition
Compared to normal meningiomas, these tumours have a faster rate of growth, which allows them to produce symptoms more quickly.
Diagnosis
Atypical meningioma diagnosis includes:
- A neurological examination evaluates the function of the brain and nerves.
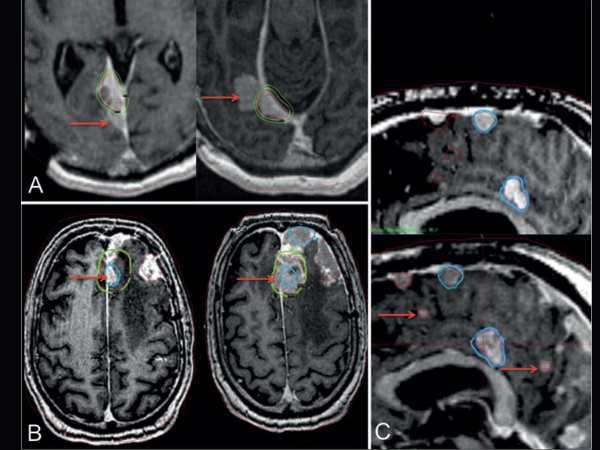
- Imaging Research:
- The preferred method for visualising tumours is magnetic resonance imaging, or MRI.
- To find any bone involvement, use a CT scan.
- Surgical resection or biopsy: for a clear diagnosis based on histological analysis.
Under a microscope, characteristics like enhanced mitotic activity, necrosis, and brain invasion aid in the tumor’s classification as atypical.
Options for Treatment
Surgery
Usually, the first course of treatment is surgical removal. Gross total resection (GTR), or the total excision of the tumour, is the aim. However, total removal might not always be feasible because of the tumor’s aggressive nature or close proximity to important brain regions.
Treatment with Radiation
After surgery, radiation is frequently utilised, particularly if:
- The tumour was not entirely eliminated.
- The tumour exhibits aggressive traits.
- Recurrence is present.
This includes more accurate choices like stereotactic radiosurgery as well as traditional external beam radiation therapy.
Radiosurgery with Gamma Knife for Atypical Meningioma
A non-invasive, highly targeted type of radiation therapy, Gamma Knife Radiosurgery (GKRS) is particularly useful in treating atypical meningiomas, specifically:
- Tumours that are found in sensitive or deep brain areas
- Tumours that remain after surgery
- Periodic meningiomas
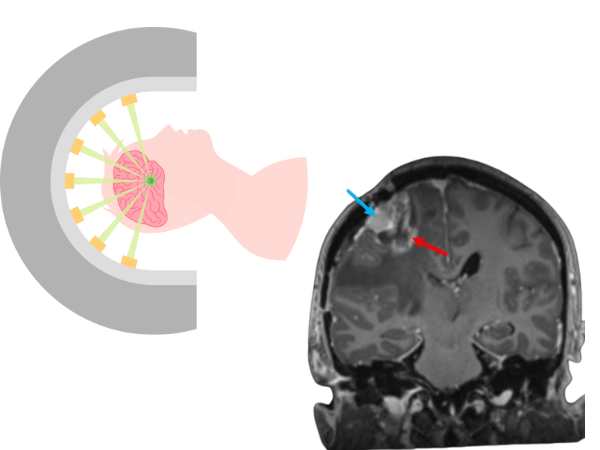
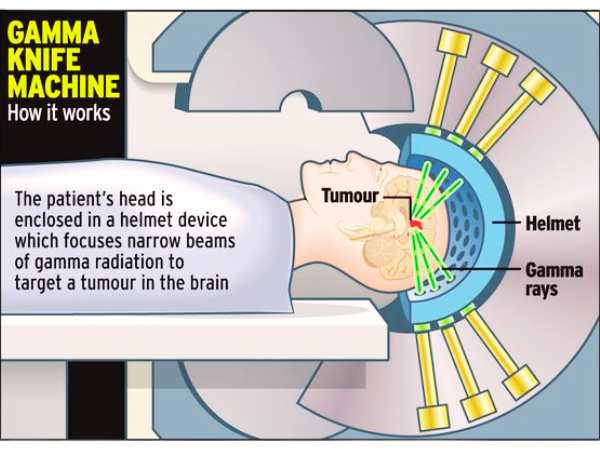
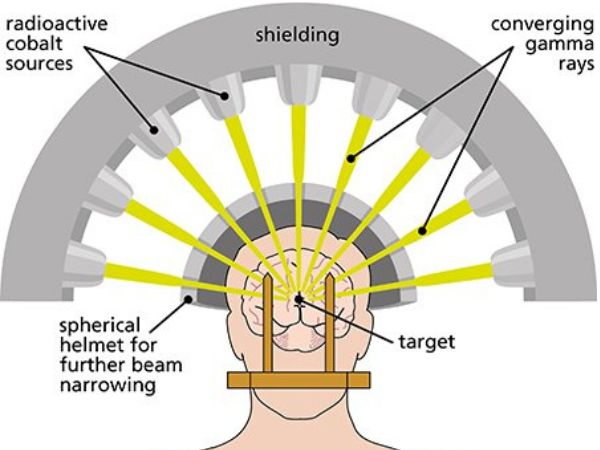
How It Operates:
- Targets the tumour with several gamma radiation beams.
- Minimally harms the healthy tissue around it.
- Usually finished without requiring a surgical incision in a single session.
Gamma Knife Radiosurgery Advantages:
- Non-invasive: neither general anaesthesia nor open surgery are required.
- Patients usually return home the same day after an outpatient operation.
- Accurate targeting lessens harm to important brain regions.
- Reduced rate of complications in contrast to traditional surgery.
- A beneficial supplement to surgery or a substitute in cases where surgery is not feasible.
Limits:
- Not appropriate for extremely big tumours.
- For tumours that are spreading quickly or are highly invasive, surgery might not be the best option.
- To determine whether there has been a recurrence or progression, long-term monitoring is necessary.
Prognosis and Follow-up
Even after total surgical removal or radiosurgery, patients with atypical meningiomas need to have regular MRI scans performed as part of a long-term follow-up. At 20% to 40% within 5 years, the recurrence rate is much higher than that of benign meningiomas.
The outcome is dependent on:
- The degree of resection
- Features of histology
- Reaction to radiation treatment
- The patient’s overall or general health
In conclusion
Because of their aggressive nature and tendency to recur, atypical meningiomas pose particular difficulties. The best possibilities for long-term control are with a mix of radiation and surgery, such as Gamma Knife Radiosurgery. It is essential to speak with a qualified neurosurgeon and a multidisciplinary team if you or a loved one has been diagnosed with an atypical meningioma in order to create a customised treatment strategy.
Please get in touch with our centre for professional treatment of atypical meningiomas, including the newest Gamma Knife technologies.
Sources:
- https://pmc.ncbi.nlm.nih.gov/articles/PMC7714950/
- https://pubmed.ncbi.nlm.nih.gov/32586495/
- https://radiopaedia.org/articles/atypical-meningioma
- https://www.pathologyoutlines.com/topic/cnstumoratypicalmeningioma.html
- https://www.sciencedirect.com/science/article/abs/pii/B9780128221983000434
- https://www.advancesradonc.org/article/S2452-1094(24)00272-0/fulltext
- https://www.sciencedirect.com/science/article/abs/pii/S1878875015013649
- https://link.springer.com/chapter/10.1007/978-3-7091-1376-9_13
- https://www.sciencedirect.com/science/article/pii/S2452109424002720
- https://www.redjournal.org/article/S0360-3016(09)01590-9/fulltext