In neurosurgery, arteriovenous malformations (AVMs) in deep brain regions such as the thalamus and basal ganglia provide a special difficulty. These areas are essential for consciousness, motor control, sensory processing, and a number of autonomic processes. There is a significant chance of neurological impairments following traditional surgical procedures in these locations. But because to developments in neurotechnology, Gamma Knife radiosurgery (GKRS) is now a very accurate and less invasive therapeutic option for these kinds of complicated lesions.
Recognising AVMs in the Thalamus and Basal Ganglia
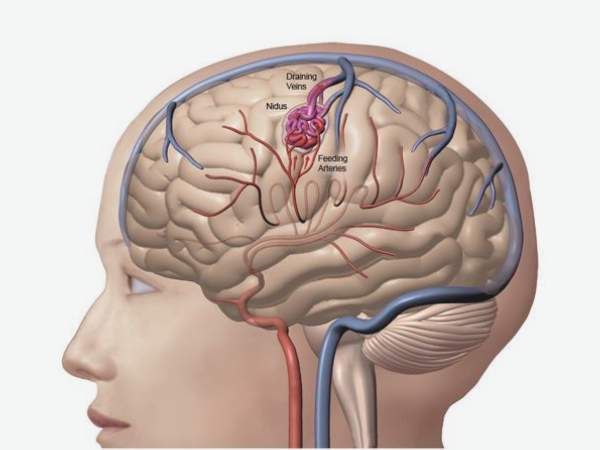
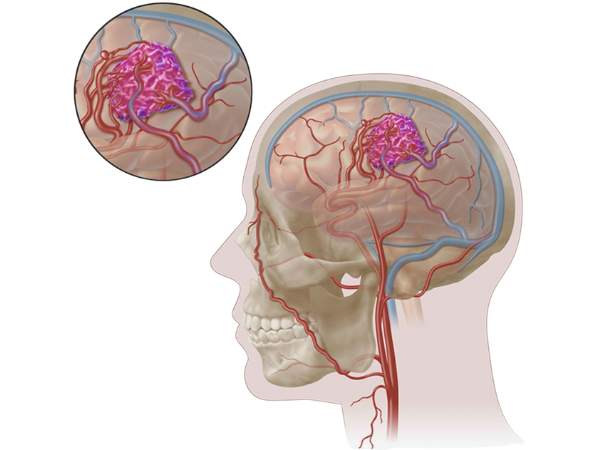
An abnormal, twisted network of blood vessels in which arteries join veins directly without going via capillaries is known as an arteriovenous malformation. Hemorrhagic stroke may result from the rupture of the vessels caused by the high-pressure blood flow created by this.
AVMs in the Basal Ganglia
The basal ganglia reside deep within the brain and play a role in cognitive and movement control. Because of the nearby important tissues, AVMs in this region are challenging to surgically approach and are frequently discovered following an unexpected haemorrhage.
AVMs that are thalamic
Sensory and motor signals are transmitted via the thalamus. Here, AVMs are frequently deeply ingrained, and intervention poses a significant risk of compromising voluntary movement, awareness, and sensory perception.
Gamma Knife Radiosurgery: What is it?

Gamma Knife Radiosurgery is a stereotactic, non-invasive radiosurgical technique that treats disorders deep inside the brain without making an actual incision by using concentrated gamma radiation beams.
- In spite of its name, it is a radiosurgical instrument rather than a knife.
- It provides more than 200 intensely concentrated gamma-ray beams that focus at one spot (the AVM nidus), giving the lesion a potent radiation dose while preserving the surrounding healthy brain tissue.
Gamma Knife for Deep-Seated AVMs: Why Use It?
In the thalamic and basal ganglia, traditional microsurgery or endovascular embolisation is frequently risky or less successful because
- This AVMs’ depth and inaccessibility.
- Proximity to eloquent regions, raising the possibility of serious brain injury.
- Complete nidus removal without resulting in irreversible impairments is difficult.
Gamma Knife Radiosurgery Benefits:
- Minimally invasive: No general anaesthesia or incision is necessary.
- High precision: AVM nidus targeting with sub-millimetric accuracy.
- Short recovery period and shorter hospital stay are two benefits of an outpatient treatment.
- Essential for deep, expressive brain regions, it preserves the surrounding brain tissue.
- Cumulative effect: Over the course of one to three years, the AVM gradually obliterates.
The Step-by-Step Process
- Imaging Prior to Surgery
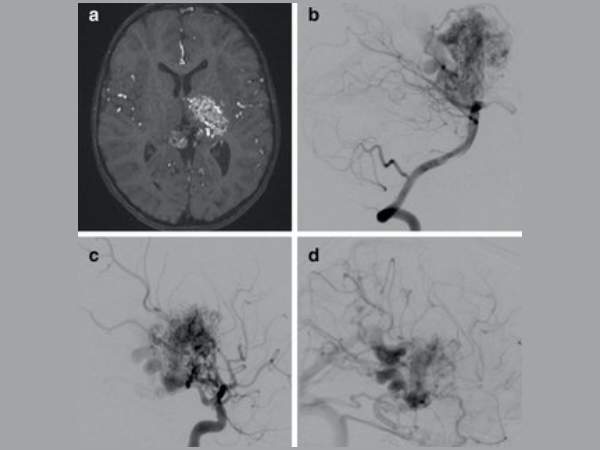
- The AVM nidus, together with its feeding arteries and draining veins, are precisely mapped using high-resolution MRI, CT Angiography (CTA), and Digital Subtraction Angiography (DSA).
- Placement of Stereotactic Frames
- To guarantee accurate targeting, a lightweight head frame is placed while under local anaesthesia.
- Planning for Treatment
- Radiation oncologists and neurosurgeons plan the precise coordinates and dose needed for the AVM using specialised software.
- Delivery of Radiation
- As the Gamma Knife equipment sends concentrated radiation beams to the AVM, the patient lays comfortably. Depending on the size and complexity of the lesion, the process can take anywhere from 30 minutes to several hours.
After Surgery Care
- After a few hours of observation, the patient is usually released that same day. A follow-up imaging procedure is planned to evaluate the development of obliteration.
Anticipated Results
- Obliteration Rates: Research on deep-seated AVMs treated with GKRS over a three-year period reveals obliteration rates ranging from 70 to 90%.
- Haemorrhage Risk Reduction: The chance of rebleeding dramatically decreases as soon as the AVM begins to diminish.
- Minimal Morbidity: There is a significantly lesser chance of neurological deterioration than with open surgery.
Hazards and Things to Think About
Even though Gamma Knife is thought to be safe, several negative consequences may still happen:
- Edema brought on by radiation: This transient swelling might result in headaches or other neurological problems.
- Although rare, radiation necrosis can cause irreversible impairments if left untreated.
- Delayed AVM rupture: Haemorrhage is still possible until complete obliteration is accomplished.
- Follow-up is necessary: Imaging must be done on a regular basis to track development.
Who is a candidate for this?
Individuals with:
- Little to medium-sized AVMs in the thalamus or basal ganglia.
- Bleeding history from a deep AVM.
- AVMs are not appropriate for embolisation or surgical resection.
- Patients who are high-risk candidates for surgery or who choose non-invasive treatment.
In conclusion
The treatment of thalamic AVMs and basal ganglia has been completely transformed by Gamma Knife Radiosurgery, which provides a non-invasive, safe, and efficient substitute for traditional neurosurgery. It gives patients with profound brain vascular abnormalities that would otherwise be incurable fresh hope because of its precise targeting and low risk of consequences.
To find out if Gamma Knife Radiosurgery is the best course of action for you or a loved one who has been diagnosed with a deep-seated AVM, speak with an experienced neurosurgeon with radiosurgery experience.
Sources:
- https://pubmed.ncbi.nlm.nih.gov/22264181/
- https://thejns.org/view/journals/j-neurosurg/116/4/article-p899.xml
- https://pubmed.ncbi.nlm.nih.gov/19415175/
- https://www.sciencedirect.com/science/article/abs/pii/S0967586815006128
- https://link.springer.com/article/10.1007/s00701-009-0335-0
- https://www.jocn-journal.com/article/S0967-5868(15)00612-8/abstract