A Glomus Jugulare Tumor: What Is It?
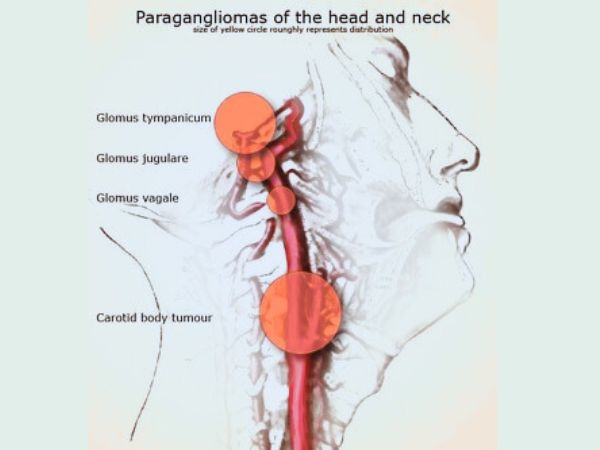
The paraganglionic cells in the jugular foramen of the temporal bone at the base of the skull give rise to an uncommon, usually benign, but locally aggressive vascular Tumor called a Glomus Jugulare Tumor. These cancers belong to a larger class of Tumors called paragangliomas, which come from the autonomic nerve system and are intimately linked to the body’s control of blood pressure and other autonomic processes.
Glomus Jugulare Tumors are generally benign (non-cancerous), but they can be extremely infiltrative, growing slowly but steadily, and can cause serious symptoms by infiltrating nearby structures like the middle ear, cranial nerves, and neck vascular structures.
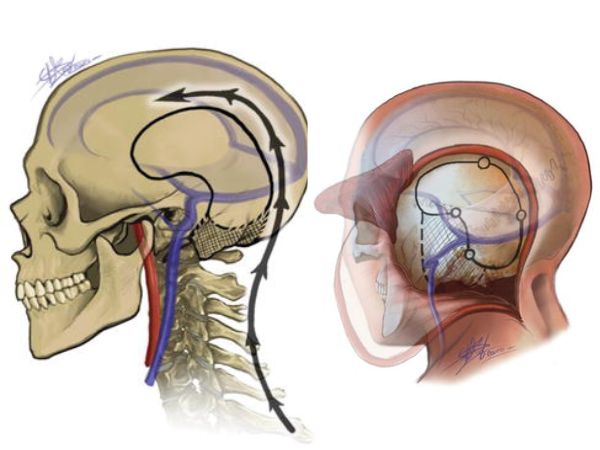
Origin and Anatomy
The internal jugular vein and the cranial nerves IX (Glossopharyngeal), X (Vagus), and XI (Accessory) leave the skull through the jugular foramen, a crucial opening near the base of the skull. The paraganglionic cells connected to the jugular bulb, a venous structure in this area, are usually the source of Glomus Jugulare Tumors.
Glomus Jugulare Tumor Symptoms
The Tumor may compress or affect nearby neurovascular structures as it grows, resulting in a range of symptoms, such as:
- Loss of hearing (often pulsatile)
- Ringing in the ears, or tinnitus
- Ear discharge or fullness
- Changes in voice or hoarseness
- Having trouble swallowing
- Weakness or paralysis of the face
- Unbalanced or lightheaded
- Palsy of the lower cranial nerves
More severe neurological impairments may result from advanced Tumors that spread into the brainstem or higher spinal cord.
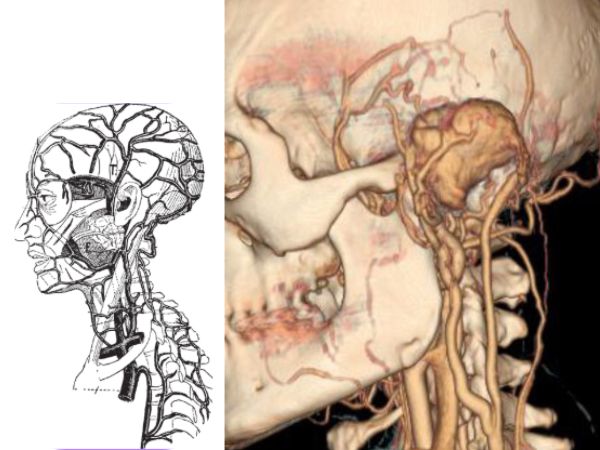
Diagnosis
A combination of imaging tests and clinical examinations is usually used to make the diagnosis, including:
- Magnetic resonance imaging, or MRI, aids in determining the tumor’s size and vascularity.
- A computed tomography (CT) scan is helpful in assessing bone degradation.
- Angiography: To view the blood supply and potentially embolise feeding vessels, it can be performed prior to surgery or before radiosurgery.
- Tests of audiometry: To evaluate hearing ability.
- Because of the vascular nature and normal radiologic appearance, a biopsy is rarely necessary.
Options for Treatment
The size, location, symptoms, age, and overall health of the patient all influence the course of treatment. The primary choices consist of:
- A remark (“Watchful Waiting”)
Imaging may be used to periodically check for small, asymptomatic Tumors in elderly or fragile patients.
- Resection via Surgery
Surgery has historically been the primary course of treatment, particularly for younger patients whose Tumors are easily accessible. However, because vital blood arteries and nerves are so close together, surgery is technically difficult and may result in haemorrhage, injury to the cranial nerve, and other problems.
- Treatment with Radiation
Tumor growth can be stopped or slowed via stereotactic radiosurgery or conventional radiation therapy.
Radiosurgery with Gamma Knife for Glomus Jugulare
Gamma Knife Radiosurgery (GKRS) is one of the most promising and less invasive methods for treating Tumors of the Glomus Jugulare. It works particularly well to prevent Tumor growth while maintaining brain function.
Gamma Knife Radiosurgery: What is it?
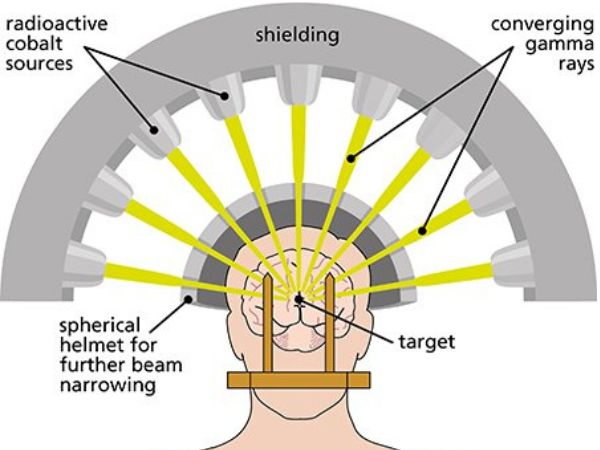
Gamma Knife is a type of stereotactic radiosurgery, radiosurgery protects the surrounding normal tissues while precisely delivering high-dose, targeted radiation to the Tumor target.
Gamma Knife Advantages for Glomus Jugulare Tumors:
- Non-invasive: No general anaesthesia or incision is necessary.
- Function preservation: A great way to preserve nerve integrity, hearing, and swallowing.
- High Tumor control rate: Research indicates that over 90% of Tumors are under control.
- Short recovery period: Patients frequently return to their regular activities in a few of days.
- Safe for inoperable cases: Perfect for patients with comorbidities or advanced age who are not suitable candidates for surgery.
- Outpatient procedure: Most of the time, no hospital stay is required.
Examples of Gamma Knife Indications:
- Tumors that are smaller than 3–3.5 cm.
- After surgery, patients with recurring or persistent Tumors.
- Unsuitable patients for open surgery.
- Tumors that affect important neurovascular structures.
Long-Term Prospects and Following
Because Glomus Jugulare Tumors develop slowly, long-term control and a high quality of life are possible with advanced treatment methods like Gamma Knife Radiosurgery. Every six to twelve months, a routine imaging follow-up (usually an MRI) is advised to check for any progression or recurrence.
In conclusion
Despite being uncommon and difficult to treat, glomus jugulare Tumors can be successfully treated by a multidisciplinary team that includes radiation oncologists, neurosurgeons, ENT experts, and radiologists. By providing a safe, efficient, and minimally invasive method that guarantees Tumor control with little morbidity, Gamma Knife Radiosurgery has completely changed the way that therapy is approached.
Sources:
- https://www.ncbi.nlm.nih.gov/books/NBK560489/
- https://pubmed.ncbi.nlm.nih.gov/32809324/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC9843021/
- https://medlineplus.gov/ency/article/001634.htm
- https://www.sciencedirect.com/science/article/pii/S2214751919303202
- https://patient.info/doctor/glomus-jugulare-Tumours
- https://journals.lww.com/neur/fulltext/2008/56010/gamma_knife_radiosurgery_for_glomus_jugulare.12.aspx
- https://thejns.org/view/journals/j-neurosurg/126/5/article-p1488.xml
- https://journals.lww.com/neurosurgery/abstract/2006/11000/gamma_knife_radiosurgery_for_glomus_jugulare.7.aspx
- https://journals.lww.com/neurosurgpraconline/Pages/instructionsforauthors.aspx