Despite its small size, the pineal area of the brain is crucial to neurological function. It can be difficult to diagnose and cure Tumors that develop in this deeply ingrained area. Treatment results have greatly improved with the introduction of sophisticated neurosurgery procedures such as Gamma Knife radiosurgery. A comprehensive explanation of pineal area Tumors, including their symptoms, diagnosis, available treatments, and the function of Gamma Knife therapy, is the goal of this article.

The Pineal Region: What is it?
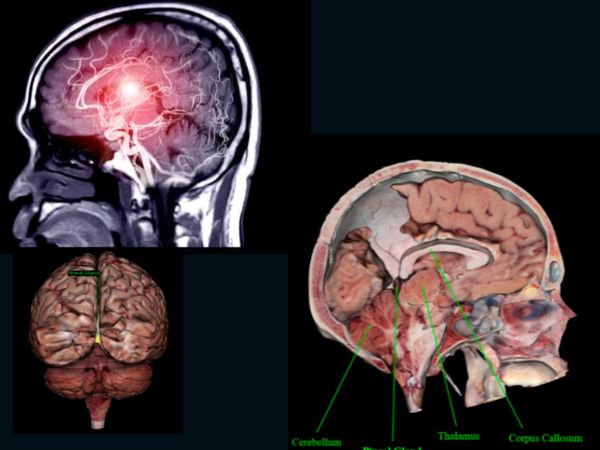
The pineal area is situated behind the third ventricle, just above the cerebellum, and between the two cerebral hemispheres, close to the centre of the brain. It contains the pineal gland, a small endocrine gland that produces the hormone melatonin, which controls circadian rhythms, or sleep-wake cycles.
Pineal Region Tumors: What Are They?
Less than 1% of all brain Tumors are pineal area Tumors, making them extremely uncommon. The pineal gland itself or nearby tissues including brain tissue, meninges, or germ cells may give rise to these Tumors.
Typical Pineal Region Tumor Types:
- The most prevalent malignant Tumor in this region is a germinoma.
- Benign and slowly developing pineocytomas
- Pineoblastomas (aggressive, high grade)
- Teratomas
- Gliomas
- Meningiomas
- Mixed germ cell Tumors and atypical Tumors
Why Do Pineal Tumors Occur?
The majority of pineal Tumors occur irregularly, which means their source is unknown.
Nevertheless, genetic changes that lead to abnormal or confused cells growing out of control can result in pineal Tumors. They may also result from abnormalities in the development of the embryo. Germ cells, for instance, usually move to develop into reproductive organs. However, some of these cells may subsequently grow into Tumors if they stay in the brain.
Even though they are uncommon, some pineal Tumors are linked to genetic disorders such as Li-Fraumeni Syndrome, which is brought on by TP53 gene abnormalities, or retinoblastoma, a rare and rapidly spreading hereditary eye cancer. Your risk of developing brain Tumors may be elevated by either of these hereditary diseases.
Pineal Region Tumor Symptoms
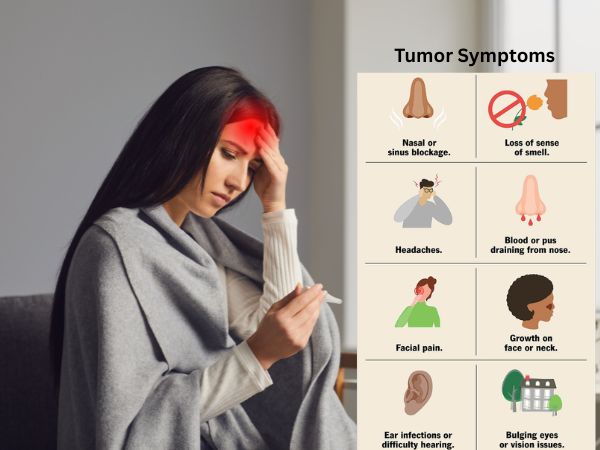
Because of the pineal gland’s deep location and close closeness to important brain areas, even small Tumors can produce serious symptoms like:
- Headache (caused by hydrocephalus or elevated intracranial pressure)
- Vomiting and feeling nauseous
- Parinaud’s syndrome, a defining feature of pineal Tumors, is the inability to move the eyes upward.
- Double or blurred vision
- Unbalanced or poorly coordinated
- Less common seizures
- Endocrine disorders (caused by melatonin or hormone pathway imbalance)
Diagnostics of Pineal Tumors
Neurological examinations, imaging studies, and laboratory work are frequently used in the diagnosis of pineal Tumors.
When diagnosing a pineal Tumor, the following instruments are frequently employed:
- Physical and neurological examination: Your doctor will first enquire about your general health, symptoms, and any potential risk factors. They will then conduct an examination to evaluate your neurological function, including reflexes, strength, coordination, sensation, and eye movements. This is because some problems with eye motions may indicate abnormalities in the pineal region.
- Ophthalmologic examination: An eye specialist may be called upon to assess your visual acuity and search for indications of elevated intracranial pressure, as pineal Tumors are known to cause symptoms connected to vision.
- The main imaging technique for detecting and diagnosing pineal Tumors is magnetic resonance imaging (MRI), which produces fine-grained images of the brain that can be used to determine the location, size, and features of a Tumor. To distinguish the Tumor from the surrounding tissues and assess its spread, an MRI with contrast may be utilised.
- Computed Tomography (CT): A CT scan uses X-rays to produce fine-grained cross-sectional brain images that aid in determining the size and location of a Tumor, even though an MRI is frequently the first option in neuroimaging. Additionally, calcifications, which are typical of pineal Tumors, and hydrocephalus can be detected using CT scans.
- A spinal tap, sometimes referred to as a lumbar puncture, is a procedure in which a needle is placed into the lower back to draw cerebrospinal fluid (CSF) in order to check for the presence of malignant cells. If your Tumor has spread throughout the central nervous system (CNS), this test can identify it.
- Blood tests: Certain pineal Tumors, especially germ cell Tumors, emit high levels of beta-human chorionic gonadotropin (hCG) or alpha-fetoprotein (AFP) in the blood or cerebrospinal fluid (CSF), which aids in the diagnosis of certain pineal Tumors.
- Biopsy: A biopsy is required if your imaging results point to a Tumor. A tiny sample is taken from the Tumor during a biopsy and sent to a pathology lab for examination. In order to identify the sort of cells present and other crucial features that inform treatment choices, pathologists there look at the tissue under a microscope. A biopsy is usually performed surgically or via stereotactic biopsy for brain Tumors.
Depending on the nature and degree of your pineal Tumor, more testing might be required.
Options for Treatment
The tumor’s nature, size, location, and grade, as well as the patient’s general condition, all influence the treatment plans.
- Observation
If small, benign Tumors like pineocytomas are not causing symptoms, they can be tracked with routine imaging.
- Resection via Surgery
- Recommended for huge, symptomatic, or accessible Tumors.
- Techniques include endoscopic, transcallosal, and infratentorial supracerebellar techniques.
- Hydrocephalus can also be relieved surgically (e.g., by conducting an endoscopic third ventriculostomy or installing a ventriculoperitoneal shunt).
- Treatment with Radiation
- Used frequently for malignant Tumors such as pineoblastomas or germinomas after surgery.
- Can be applied as the main course of treatment for some Tumors that are susceptible to radiation.
- The use of chemotherapy
- Very useful for germ cell Tumors.
- Frequently used in combination with radiation therapy for a better outcome.
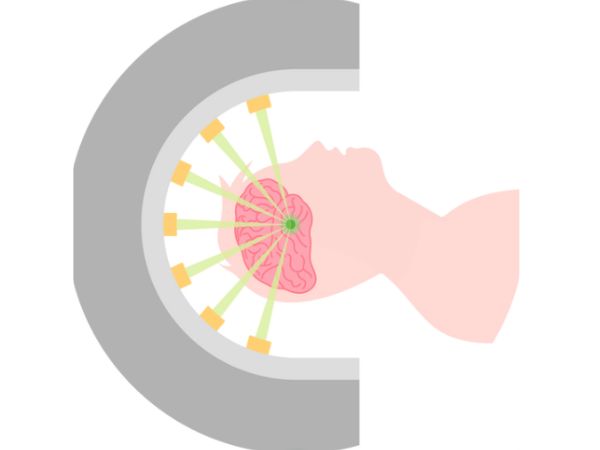
Gamma Knife in Tumors of the Pineal Region
A non-invasive therapeutic method called Gamma Knife radiosurgery uses concentrated gamma radiation beams to target brain Tumors with sub-millimeter precision. It works particularly well for Tumors that are deep, difficult to access, or still present in the pineal region.
Gamma Knife Radiosurgery Advantages:
- Minimally invasive: doesn’t require general anaesthesia or incisions.
- Targeted precisely: Preserves the area around healthy brain tissue.
- Quick recovery: Frequently carried out as an outpatient operation.
- Perfect for little or persistent Tumors following surgical excision.
- Low incidences of complications.
Gamma Knife Indications for Pineal Tumors:
- Tumors that are inoperable or inaccessible during surgery.
- Unsuitable patients for open surgery.
- Recurring Tumors following the first radiation or surgery.
- Tumor tissue that remains after partial resection.
- Adjunct therapy for low-grade gliomas, meningiomas, and pineocytomas.
Restrictions:
- Not appropriate for big Tumors that cause hydrocephalus or a substantial bulk effect.
- Delayed Tumor shrinkage—it could take weeks or months to see results.
The outlook
Depending on the form and grade of the Tumor, the prognosis for pineal area Tumors varies greatly:
- With combination chemotherapy and radiation, germinomas have a very good prognosis (cure rates of over 90%).
- When removed surgically, pineocytomas have a favourable prognosis.
- Despite multimodal treatment, high-grade gliomas and pineoblastomas have a guarded prognosis and are more aggressive.
- Results are greatly enhanced by early diagnosis and individualised therapy, including radiosurgery.
In Conclusion
Despite being uncommon, pineal area Tumors necessitate a comprehensive approach from radiation specialists, neurosurgeons, neuro-oncologists, and radiologists. Patients now have access to precise, efficient, and minimally invasive choices thanks to advancements like Gamma Knife radiosurgery, which improves survival and quality of life.
Better results may result from early evaluation by a specialised neurosurgery team if you or a loved one has been diagnosed with a pineal area Tumor. To deliver individualised, evidence-based care, AIIMS Delhi is equipped with cutting-edge diagnostic and therapeutic instruments, such as Gamma Knife technology.
Sources:
- https://pmc.ncbi.nlm.nih.gov/articles/PMC8036741/
- https://www.cancer.gov/rare-brain-spine-tumor/tumors/pineal-region-tumors
- https://www.ncbi.nlm.nih.gov/books/NBK560567/
- https://www.barrowneuro.org/condition/pineal-tumors/
- https://www.webmd.com/brain/what-to-know-about-pineal-tumors
- https://emedicine.medscape.com/article/249945-overview?form=fpf
- https://www.cancerresearchuk.org/about-cancer/brain-Tumors/types/pineal-region-Tumors
- https://radiopaedia.org/articles/pineal-region-mass
- https://pmc.ncbi.nlm.nih.gov/articles/PMC4617952/
- https://pubmed.ncbi.nlm.nih.gov/18081477/
- https://www.jkns.or.kr/journal/view.php?number=1820
- https://www.jkns.or.kr/upload/pdf/0042006160.pdf